



 Glioma
Glioma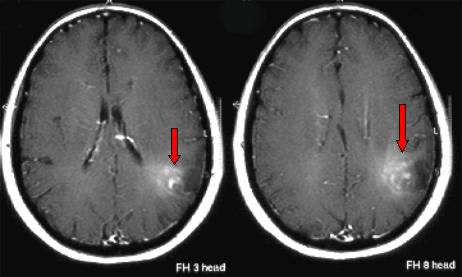
Fig.5.13: MRI of a left parietal oligodendroglioma (red arrows), with some astrocytoma components.
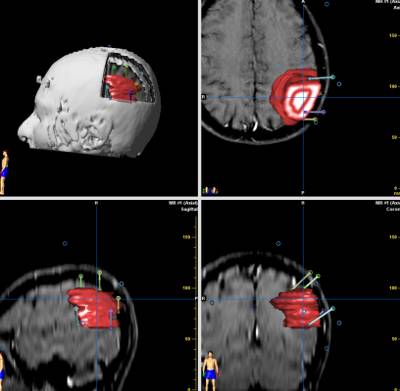
Fig.5.14: Same case at the neuronavigator (tumor in red), permitting to select the best trajectory.

Fig.5.15: Thanks to available data, the tumor is surgically isolated under the operating microscope and then removed (in this lucky case, en bloc). Bottom right: the removed tumor.
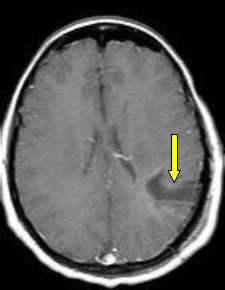
Fig.5.16: Post-operative MRI showing "total" removal of the glioma. The arrow points to the trajectory and to the residual cavity.
Oligodendroglioma is a rather chemo-sensitive brain tumor, i.e. it responds to chemotherapy better than other gliomas. The study of the tumor genes permits a good prediction of the chemo-sensitivity of this type of tumors.
There are several chemotherapeutic protocols; the most popular and effective ones are based on a combination of Procarbazine, Vincristine and CCNU (PCV) and on the use of Temozolomide alone or with radiotherapy.
Gliomas, with all their biological variations, may occur also in the spinal cord. Astrocytomas of the spinal cord are diffuse and generally difficult to remove. For their diagnosis, MRI is indicated. Gliomas of the spinal cord are rare. Surgical exploration may be indicated, as post-operative clinical worsening is a frequent occurrence. Sometimes, very good surgical results may be obtained (see next paragraph).
Page 14
 Previous Page
Previous Page
