This is a slow-growing benign tumor originating from the cells which line the vessels of the
brain or of the
spinal cord. It frequently has a cystic component along with a red, fleshy, hemorrhagic component. The walls of the cyst are generally non-tumoral. Its most common locations are
cerebellum and spinal cord. Hemangioblastomas account for about 2% of brain tumors. They may be multiple in case of a genetic illness: Hippel-Lindau. Hemangioblastomas also occur in the liver, retina, kidney.
Cerebellar hemangioblastomas present with gait disturbances,
hydrocephalus and
intracranial hypertension. Spinal cord hemangioblastomas present with slow-worsening paraparesis or tetraparesis.
The diagnosis with
MRI is quite easy as their picture is typical. In the spinal cord, selective angiography may be indicated before surgery.
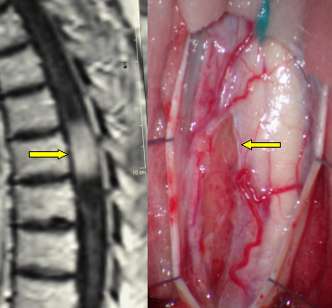
Fig. 5.22: Lateral view of MRI displaying a dorsal hemangioblastoma of the spinal cord. On the right, the incised cord under the operating microscope and the tumor that is pointed by the arrow.
Therapy is microneurosurgical removal. The solid part of the tumor must be removed, which may be technically demanding, as it is rather hemorrhagic. Spinal cord hemangioblastomas, if not too large, may be removed with
mininvasive approaches, i.e. bone demolition of the spine is minimized, avoiding all problems connected with late spine instability.

Fig. 5.23: This is the operative view of the spinal cord after removal of the tumor.
This a heterogeneous group of tumors, classified according to their location in the pineal region, behind the III ventricle. They are difficult to be operated upon because of their deep location. There are germ cell tumors that are very radiosensitive and whose diagnosis is done with
CSF markers and without biopsy. Germ cell tumors are more frequent in pediatric age; they may diffuse along the entire central nervous system; thus an appropriate study is important.
Non-germ cell tumors include teratomas, chorioncarcinomas, tumors originating from the pineal cells, gliomas originating from the upper part of the brainstem.
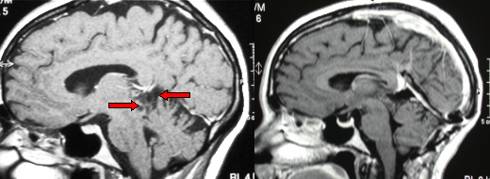
Fig. 5.24: MRI of a low-grade astrocytoma of the pineal region (red arrows). Right: view after total removal via a supracerebellar approach.
These tumors generally present with
hydrocephalus due to obstruction of the Sylvian aqueduct. The blockage may be removed by inserting an artificial system or by performing an endoscopic III ventricle-cisternostomy through a simple frontal hole (see endoscopy).
Surgical removal is technically demanding because of the deep location and of the important veins that surround the tumor in the pineal region. A good angiographic
MRI is mandatory. There are several approaches to the pineal region, each of which has advantages and disadvantages.




 Glioma
Glioma Previous Page
Previous Page
