



 Supraorbital Approach
Supraorbital ApproachMININVASIVE NEUROSURGERY
Neurosurgical departments with the philosophy of technical innovation may use mininvasive approaches in brain tumor and spinal cord tumor neurosurgery. This philosophy is based on the concept of obtaining the same or even better results than using conventional approaches. It must be kept in mind that mininvasive neurosurgery should not be used as a technical exercise.The Central Nervous System (CNS) is contained in a bony-ligamentous box. To gain access, this box must be opened. The opening of the "box" is minimized in mininvasive neurosurgery. For brain tumors, the contrary may be true, i.e. for some tumors of the cranial base, the "box" must be widely opened to permit safe access to its deep structures. Thus, mininvasive neurosurgery for brain tumors and spinal cord tumors should be used under well-established criteria and in selected cases, otherwise a clinical disaster may be expected.
In the Neurosurgical Division of the "Regina Elena" National Cancer Institute, some mininvasive techniques are used whenever possible, thanks also to the use of modern operative technologies.
This is an elegant way to access the anterior cranial base brain tumors: meningioma of the planum sphenoidale, ethmoidal meningioma, tuberculum sellae meningioma, craniopharyngioma. An incision is made on the supraorbital rim and a small bony window is cut (2x3 cm). The key is correct patient positioning, which permits the frontal lobe to be gently displaced to reach the operating field. A great advantage is that these patients do not need any antiepileptic drugs, as the brain has practically no contusion. The cosmetic results are excellent. Another advantage is that the temporal muscle is not damaged, as in lateral approaches, thus avoiding the frequent chewing problems and post-operative pain.
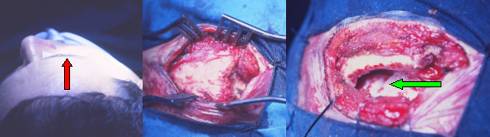
Fig.7.1: From left, skull positioning, incision over the supraorbital rim (red arrow), exposure of the bone, cutting of the small flap. The green arrow points to the dura mater, which will be cut to enter the intradural space.
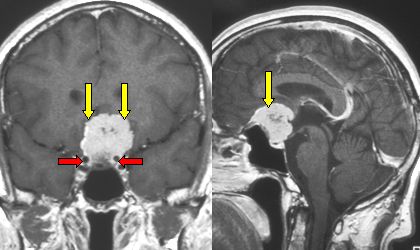
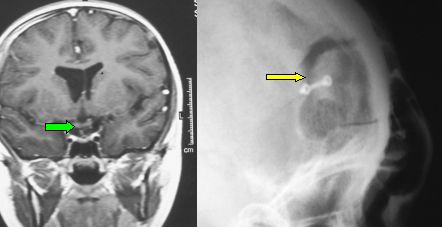
Fig.7.2: Same case as in Figs. 5.33 and 5.34. The red arrows identify the internal carotid arteries. Bottom right: the small bone flap that has been repositioned and fixed with titanium microplates. Bottom left: post-operative MRI; the green arrow points to the optic chiasm.
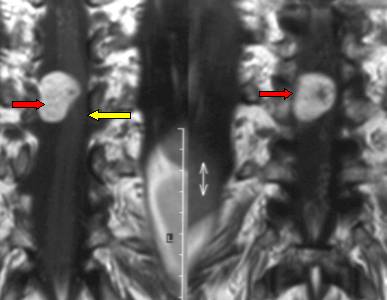
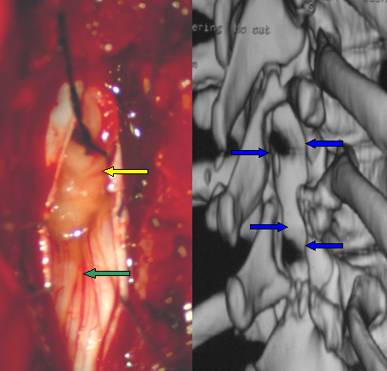
Fig.7.3: Above, frontal MRI of a rather large neurofibroma (neurinoma, schwannoma) compressing the low dorsal cord at D10-D11; the red arrows point to the tumor, the yellow one to the cord. Bottom left, intra-operative view of the tumor (yellow arrow), cord and cauda equina (green arrow), as seen from this mininvasive approach. Limited bone removal may be seen on the 3D-reconstructed CT Scan taken post-operatively (bottom right).
Page 28
 Previous Page
Previous Page
