



 Operating Microscope
Operating MicroscopePreviously collected MRI or CT Scan data are fed to the neuronavigator. Sensors are applied on the patient's skull. Other sensors are matched with surgical instruments. In the operating room, there is a double antenna (equivalent to GPS satellites) and a screen with the map of the particular brain tumor. The brain appears on the screen and/or directly in the operating microscope oculars. The trajectory to the lesion is safely guided by the neuronavigator.

Fig.6.2: In the foreground, the neuronavigator; in the back, our old ZEISS NC4, which has been replaced by the more modern Pentero.
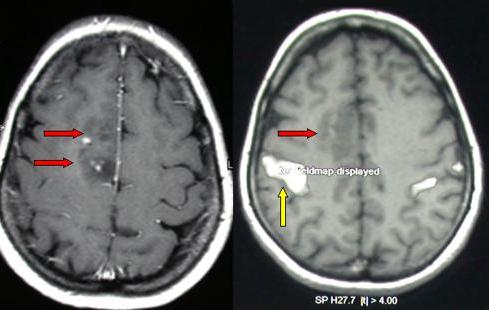
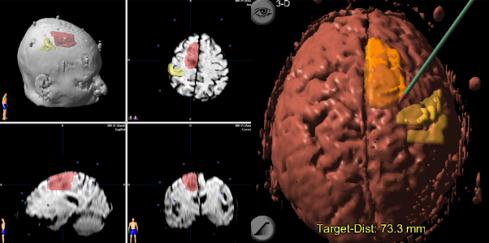
Fig.6.3: This picture explains how the neuronavigator works in routine use. Upper left: right frontal astrocytoma (red arrows) quite close to the motor area, as seen on functional MRI (upper right, yellow arrow). In neuronavigation (bottom left), the tumor is shown in red and the motor areas in yellow. Bottom right: trajectory displayed on the neuronavigator screen; the margins of the lesions, as well as their relationships with the motor area are well depicted (the operating room equipment gives direct images, i.e. right is right and left is left).
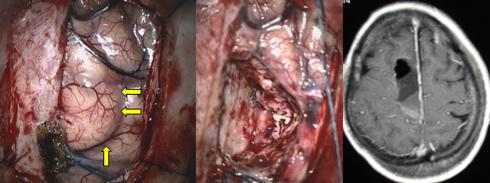
Fig.6.4: Thanks to the neuronavigator, the surgeon cuts a precise "wedge" of the affected tissue and spares the surrounding healthy brain. Center: the "hole" after brain tumor removal. Right: MRI taken the day after surgery.
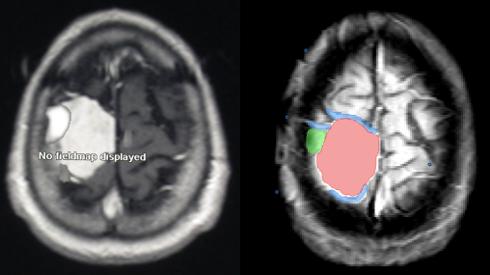
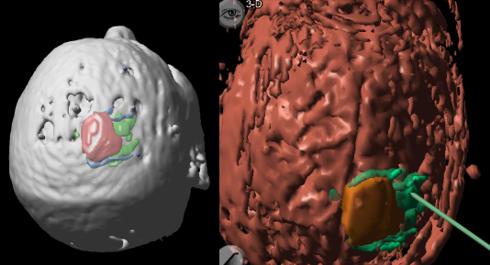
Fig.6.5: The neuronavigator is also helpful in meningioma surgery. In this case, the tumor is pink, the motor area is green and the important cortical veins are blue.
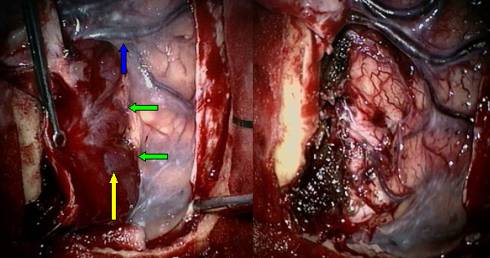
Fig.6.6: Upon surgery, the data from the neuronavigator prove to match the real anatomy. On the left, the meningioma (yellow arrow), while it is being detached from the underlying brain, having care to preserve the veins (blue arrow). The green arrows points to the cleavage plane between the brain and the meningioma. On the right, the removal has been completed and the veins have been spared.
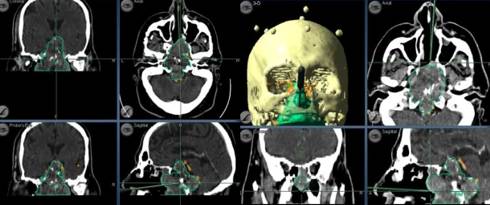
Fig.6.7: Same case as in Figs. 5.54 and 5.55. The neuronavigator coupled with CT Scan permits intra-operative definition of the borders of the tumor.
Page 26
 Previous Page
Previous Page
