This is a rare tumor (less than 1% of brain tumors). It is some more frequent in infancy. It originates from the epithelial cells which line the choroid plexus of the ventricles, where the
CSF is produced. Papillomas are mainly located in the lateral ventricles and cause
hydrocephalus and
intracranial hypertension.
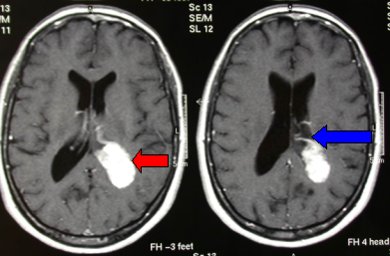
Fig. 5.25a: Left posterior intraventricular papilloma (red arrow); the blue arrow points to the major feeding artery.
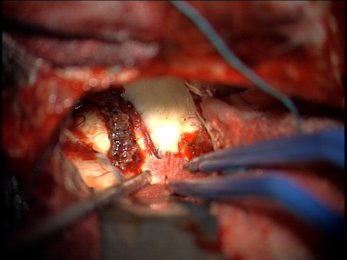
Fig. 5.25b: Intra-operative view of the same case under the operating microscope. The last piece of the papilloma is the one in the forceps.
Surgery is important. Papillomas are deep-seated tumors and the approach must be chosen on the basis of
functional MRI and angiography findings. In the presented case (Fig. 5.26,27), the transcortical approach was avoided (dominant hemisphere) and a posterior parasplenial trajectory was chosen.
There is also a very rare malignant type: plexus carcinoma.
Other intraventricular tumors
Also
gliomas and
meningiomas may be intraventricular. Gliomas that grow into the ventricles are not rare: they may originate from the thalamus or the anterior basal ganglia. Intraventricular meningiomas are very rare.
Intraventricular tumors may reach huge dimensions, as they grow in a free space. They present with intracranial
hypertension and
hydrocephalus, which is an early symptom due to obstruction of the
CSF pathways.
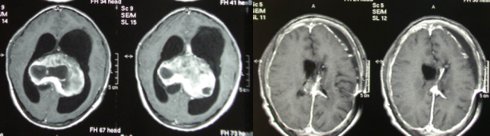
Fig. 5.26: Above, pre-operative MRI of a giant pilocytic astrocytoma (9 cm); below, MRI taken six months post-op and showing removal of the tumor and treatment of hydrocephalus with an artificial system.
These are rare and
benign tumors, consisting of fat. They are the result of a malformation. Fat is included in the CNS in the early stages of its formation and lipomas may grow from these fat cells. In the brain, their typical location is the corpus callosum. Generally, these tumors are incidentally found upon
CT or
MRI done for other reasons. They do not need any therapy.
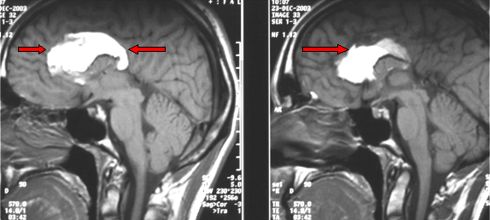
Fig. 5.27: MRI of a typical case of corpus callosum lipoma.
There are also
lipomas of the spinal cord, which have the same growing mechanism. They are located in the most caudal part of the cord or at the filum terminale. They become symptomatic in young people during growth, as the presence of the lipoma blocks the cord in its natural upward migration. Thus, deficits of the feet and sphincteric problems may occur owing to stretching of the cord. In these cases, the therapy is microneurosurgery with partial removal of the lipoma and resection of the scars that prevent the upward migration of the cord (tethered cord syndrome).




 Glioma
Glioma Previous Page
Previous Page
