



 Glioma
Glioma5.3 High-grade astrocytoma - Glioblastoma Multiforme
These are the malignant and very aggressive types of astrocytoma (Grade III and IV of the WHO classification). Grade IV is generally called glioblastoma multiforme.
The histological classification is performed on the most malignant part of the removed tissue. Part of the tumor may recall a low-grade glioma; if even small areas of degeneration are present, the tumor will be classified as malignant.
High-grade gliomas may be multicentric, i.e. with separate pathological areas in the brain
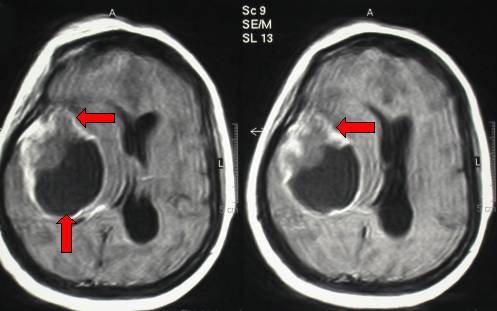
Fig.5.9: Typical right temporal glioblastoma upon axial MRI. The image is of bad quality, because the patient was agitated due to severe intracranial hypertension. The operation was completed within few hours.
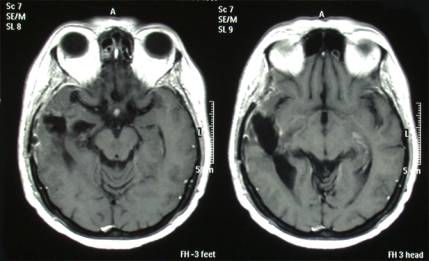
Fig.5.10: Post-operative MRI of the same patient. Despite "gross total removal", radio- and chemotherapy, this gliobastoma recurred at 14 months and the patient died at 22 months.
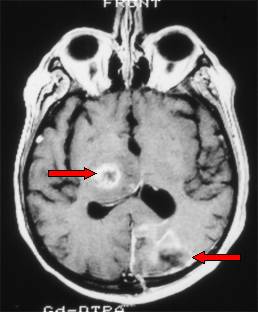
Fig.5.11: Multicentric glioblastoma upon the first diagnosis (the arrows point to two separate tumoral areas).

Fig.5.12: This is the operating room with the positioned patient, the neuronavigator and the operating microscope.
For details, see Chapter 6: "Modern Operative Technologies".
Radiotherapy is indicated after operation. Modern techniques, e.g. conformational and stereotactic radiotherapy, offer "good" results with fewer complications than before. Aggressive chemotherapy with temozolomide is the first choice, particularly if the glioma cells are methylated. Other second-line treatments are available but unfortunately they do not cure these patients. The median survival in grade III astrocytomas is 24-36 months, 12-18 months in glioblastoma.
A second operation may be indicated at recurrence, followed by radiotherapy again, where practicable.
Antiepileptic medication associated with corticosteroids may assure a good quality of life to these unfortunate people. Other crucial operators are: physiotherapists, psychologists, neuroncologists. The patient with malignant brain tumor should not be abandoned. If correctly treated, his/her quality of life will be rather good and with lower expenses for his/her family and/or the national health care system.
Page 13
 Previous Page
Previous Page
