Metastatic brain tumors, i.e. intracranial masses secondary to tumors arising in other parts of the body, are the most frequent. Those that more commonly involve the
brain are: lung, breast and gastrointestinal tract carcinomas, as well as melanomas. At times, brain metastases are the only sign of cancer: a silent primary tumor; this is rather frequent in lung carcinomas and melanomas.
The occurrence of brain metastases is a severe event in case of "cancer". It means that the disease is disseminated and that the brain, a vital organ, is the target of this dissemination.
Brain metastases present with
seizures and focal neurological deficits, depending on their location. Rarely, they are clinically silent and discovered in their early stages during
CT scan follow-up of cancer patients.
Brain metastases cause major tissue suffering: edema. Brain metastases are often multiple. In these instances, they may cause a severe intracranial
hypertension syndrome.
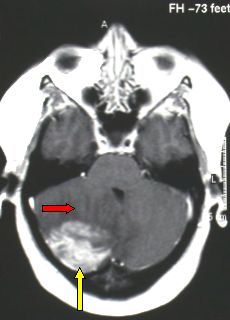
Fig.5.50: Axial MRI view of large right cerebellar metastases (yellow arrow) with severe perilesional edema (red arrow).
Neurosurgical removal is probably the most rapid and effective treatment, when the lesion is single and with important clinical signs, provided that its location is favorable. The results are often dramatically good in very few days. This is an important parameter for people who do not have long life expectancy. Therapy for metastases is palliative and not curative.
Modern operative technologies are of help:
neuronavigation and echography are crucial to identifying small lesions or demarcating the boundaries of large lesions.
Neuronavigator combined with functional
MRI permits to avoid critical brain areas.
If the surgical indication is correct, results are very good.
Radiosurgery is an effective alternative in brain metastasis treatment. It is crucial for multiple small lesions, which can be treated simultaneously. In our opinion, it should not be used as the therapy of choice for surgically removable single metastases. Radionecrosis is not infrequent after radiosurgery. Patients should also receive high-dose corticosteroids for a long time after treatment. Thus,
radiosurgery should be confined to deep-seated single brain metastases and, obviously, to multiple lesions.
Whole Brain Radiotherapy (WBRT) is done after removal of a single brain metastasis. It is an attempt to prevent recurrence or occurrence of other metastases in different sites.




 Glioma
Glioma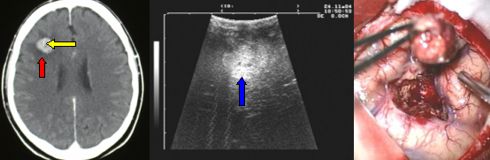
 Previous Page
Previous Page
