



 Supraorbital Approach
Supraorbital Approach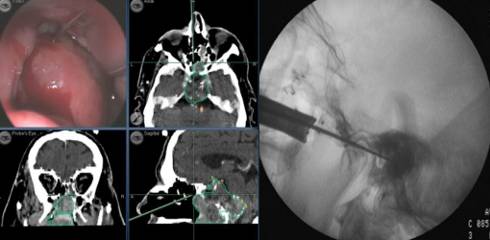
Fig.7.4: Same case as in Figs. 6.7, where the endoscope is matched with the neuronavigator. In the direct transnasal approach, the retractor is inserted directly from the nostril to the anterior wall of the sphenoid, without septal dissection.

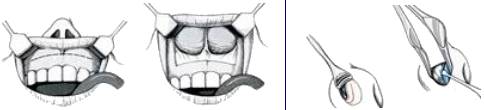
Fig.7.5: Above left, the traditional sublabial route; on the right, the nasal-transeptal approach. Bottom left, anatomical view of the transphenoidal route to the pituitary (arrow). These more conventional operations may cause some nasal and dental complications.
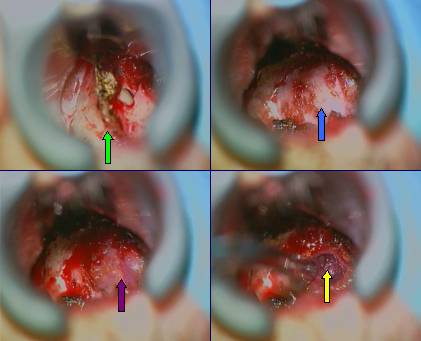
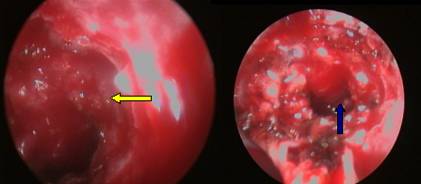
Fig.7.6: Operative sequence of mininvasive direct transnasal approach to a pituitary adenoma. From left to right and from top to bottom: under microscopic vision, the retractor has been inserted up to the sphenoid sinus, which is opened (green arrow); the floor of the sella has been removed, exposing the pituitary dura (blue arrow); once the dura has been opened, the pituitary adenoma appears in the operating field (violet arrow) and may be removed (yellow arrow). The endoscope permits to find hidden portions of the tumor (yellow arrow). Bottom right, blue arrow pointing to the final operating field.
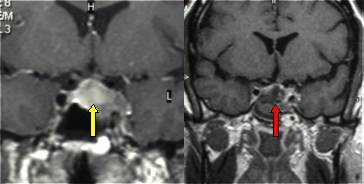
Fig.7.7: Left, pre-operative frontal MRI of this pituitary adenoma yellow arrow). Right, post-operative MRI taken within 24 hours. The red arrow points to the residual hole.
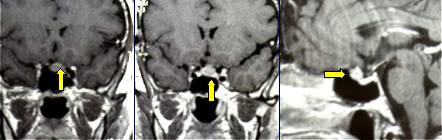
Fig.7.8: Frontal and lateral MRI views of a small recurrent tuberculum sellae meningioma (yellow arrow), which may be accessed via the endoscope-assisted direct transnasal approach.
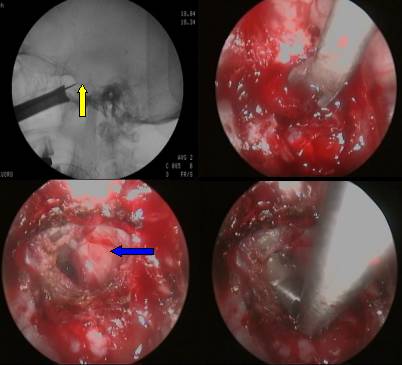
Fig.7.9: Operative sequence of the same case. Above left, centering of the sella (yellow arrow). Right, the tumor being removed under endoscopic vision. Bottom left, exposure of the optic chiasm after tumor removal (blue arrow). Bottom right, articulated mirror showing the most hidden portions of the field.
Page 29
 Previous Page
Previous Page
